What a Chinese study on sodium hyaluronate plus hydroxyapatite microspheres suggests
Periorbital rejuvenation, particularly in the lower-eyelid and tear-trough region, is one of the more difficult areas in injectable aesthetics. Compared with the midface, nasolabial folds, or jawline, this area has thinner skin, more delicate tissue layers, and a stronger visual impact from vascular show-through, pigmentation, infraorbital volume change, and soft-tissue support.
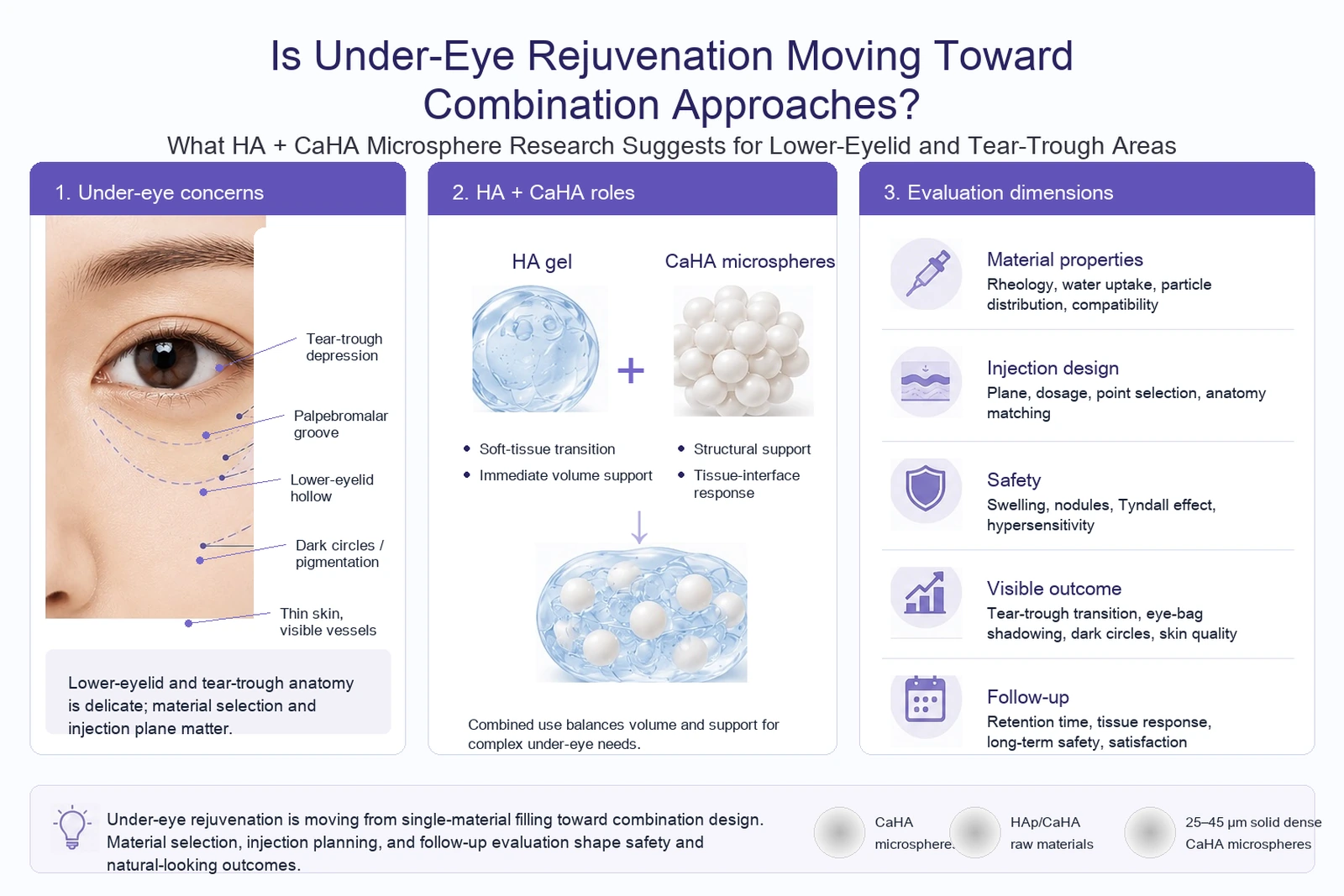
The concern is rarely a single hollow. Tear-trough depression, palpebromalar groove visibility, infraorbital shadowing, dark circles, and skin-texture changes may appear together. Material selection, injection plane, dosage control, and follow-up observation all affect how the result is evaluated.
In recent literature, the combined use of hyaluronic acid (HA) and hydroxyapatite microspheres (CaHA microspheres) has started to appear in more discussions around the lower eyelid and tear trough. This does not mean one material is replacing another. It suggests that under-eye rejuvenation is moving from single-material volumization toward more specific combination approaches.
A 2026 article in Chinese Journal of Aesthetic Medicine, titled Application of Injectable Sodium Hyaluronate Combined with Hydroxyapatite Microspheres in Lower Eyelid Rejuvenation, addressed this direction. The study included 84 subjects seeking injectable treatment for lower-eyelid aging and compared sodium hyaluronate combined with hydroxyapatite microspheres against sodium hyaluronate alone.
Why lower-eyelid assessment is not just about volumization
Changes in the lower eyelid and tear-trough region usually come from several factors at the same time. Infraorbital volume loss can create a hollow. The lid-cheek junction can deepen the shadow. Thin skin or vascular show-through can make dark circles more visible. Soft-tissue laxity can also affect the transition around the eye.
This is why under-eye volumization is not simply a matter of adding volume to a depression. Superficial placement, excessive volume, or strong water uptake may contribute to swelling, optical issues, or an unnatural contour. Insufficient support may fail to address deeper volume loss or structural transition.
The HA-CaHA microsphere combination is worth discussing in this context because the question is not only how much material is placed. The more relevant question is how the gel phase, particulate phase, injection plane, and tissue response work together.
What HA and CaHA microspheres contribute in a composite system
Sodium hyaluronate is widely used in injectable volumization and soft-tissue augmentation. It is often used for volume restoration, soft-tissue transition, and local contour adjustment. Different crosslinking levels and rheological profiles allow HA gels to be designed for different handling and placement requirements.
Hydroxyapatite microspheres are a calcium-phosphate particulate phase. In a composite system, CaHA microspheres are not simply a filler-particle label. Particle-size distribution, sphericity, particle integrity, surface state, phase composition, and dispersion behavior can all influence later formulation evaluation and product verification.
The useful question is therefore not which material is better. A more practical reading is that HA provides the gel matrix and volume support, while CaHA microspheres introduce a particulate phase that needs to be evaluated for distribution, structural behavior, and tissue-interface response. In a sensitive area such as the lower eyelid, this division of roles matters more than the phrase combination treatment itself.
What the lower-eyelid study reported
According to the public abstract, the study included 84 subjects with lower-eyelid aging who visited the clinic between September 2022 and June 2023. The study group included 42 subjects treated with sodium hyaluronate plus hydroxyapatite microspheres, while the control group included 42 subjects treated with sodium hyaluronate alone. In the original Table 1, the baseline-characteristics comparison was reported for 41 subjects in the study group and 40 subjects in the control group. Sex, age, and total injection volume did not differ significantly between groups. The mean ages were 32.13 ± 13.25 years and 33.09 ± 13.34 years, and total injection volumes were 0.91 ± 1.12 ml and 0.96 ± 0.98 ml, respectively.
| Variable | Study group (n=41) | Control group (n=40) | Significance |
|---|---|---|---|
| Age (years, mean ± SD) | 32.13 ± 13.25 | 33.09 ± 13.34 | Not significant |
| Total injection volume (mL, mean ± SD) | 0.91 ± 1.12 | 0.96 ± 0.98 | Not significant |
| Sex distribution | No significant difference between groups | — | |
The original Table 2 listed the devices and materials used in the study, including hydroxyapatite bioceramic material (S type), injectable cross-linked sodium hyaluronate gel, compound lidocaine cream, and sharp and blunt needles. For material development, this table matters because it shows that the paper evaluated a specific injection protocol, not an abstract HA plus CaHA concept.
| Category | Item |
|---|---|
| Particulate phase | Hydroxyapatite bioceramic (S type) |
| Gel phase | Injectable cross-linked sodium hyaluronate gel |
| Topical anesthesia | Compound lidocaine cream |
| Injection devices | Sharp needles and blunt cannulas |
The tear-trough and palpebromalar-groove score was one of the main endpoints. In the original Table 3, the study-group score decreased from 3.33 ± 0.92 before treatment to 2.01 ± 0.39 at 6 months. The control-group score decreased from 3.46 ± 0.88 to 2.19 ± 0.49. Within-group changes were significant in both groups (P<0.001). Between groups, baseline scores did not differ significantly, while the 6-month score was lower in the study group (P=0.036).
| Group | Baseline | 6 months after treatment | Within-group P |
|---|---|---|---|
| Study group (n=41) | 3.33 ± 0.92 | 2.01 ± 0.39 | <0.001 |
| Control group (n=40) | 3.46 ± 0.88 | 2.19 ± 0.49 | <0.001 |
| Between-group P | Not significant | 0.036 | — |
The dark-circle score showed a clearer separation between groups. In the original Table 4, the study-group score decreased from 2.26 ± 0.71 to 1.57 ± 0.38 (P<0.001). In the control group, the score changed from 2.12 ± 0.78 to 1.98 ± 0.87 (P=0.225). The between-group comparison at 6 months was significant (P=0.004). Within the scoring framework of this paper, the combination group therefore showed a more evident reduction in dark-circle score.
| Group | Baseline | 6 months after treatment | Within-group P |
|---|---|---|---|
| Study group (n=41) | 2.26 ± 0.71 | 1.57 ± 0.38 | <0.001 |
| Control group (n=40) | 2.12 ± 0.78 | 1.98 ± 0.87 | 0.225 |
| Between-group P | — | 0.004 | — |
Complications also need to be read together with the score data. The original Table 5 reported 1 case of ecchymosis, 1 allergic reaction, 3 cases of nodule or cord-like elevation, and 1 case of overcorrection in the study group, with no infection, undercorrection, or Tyndall phenomenon. In the control group, the table reported 1 allergic reaction, 1 case of nodule or cord-like elevation, 1 case of undercorrection, and 4 cases of Tyndall phenomenon. Because the sample size was limited, these data are best read as observations within this study protocol, not as a general safety conclusion for all under-eye HA-CaHA systems.
| Complication | Study group (n=41) | Control group (n=40) |
|---|---|---|
| Ecchymosis | 1 | 0 |
| Allergic reaction | 1 | 1 |
| Nodule or cord-like elevation | 3 | 1 |
| Overcorrection | 1 | 0 |
| Undercorrection | 0 | 1 |
| Infection | 0 | 0 |
| Tyndall phenomenon | 0 | 4 |
These results make the discussion more concrete. Tear-trough and palpebromalar-groove scores, dark-circle scores, and complication types formed the main evaluation frame used by the original paper. Compared with nasolabial folds, the midface, or contour shaping, the under-eye region is more sensitive to rheological behavior, injection depth, particle distribution, and post-treatment reaction.
The boundary is also important. This is a clinical observation from a specific publication, with a defined sample size and a 6-month follow-up period. It should not be read as evidence that every HA-CaHA combination is suitable for the under-eye region, nor should it replace independent evaluation across products, patient groups, injection planes, and protocols.
Combination approaches are not about adding more material
In the under-eye area, a combination approach does not mean a more aggressive treatment concept. It asks for a more precise one.
Lower-eyelid rejuvenation often involves volume, support, skin texture, and light-shadow transition at the same time. A single material may not cover every issue, but a combination approach is not simply the stacking of multiple materials in one area. The important questions are how the gel phase and particulate phase are distributed, whether the material matches the intended plane, whether local reactions can be controlled, and whether the observed change remains stable during follow-up.
In this study, HA plus CaHA microspheres were not evaluated only by whether a hollow could be corrected. The paper also looked at tear-trough and palpebromalar-groove scores, dark-circle score, and complication categories. In the under-eye region, visible quality, stability during follow-up, and local reactions all affect how a protocol is judged.
What this means for CaHA microsphere development
For CaHA microsphere development, the main takeaway from this type of study is not a single clinical conclusion. The more relevant point is that composite systems place clear requirements on hydroxyapatite microspheres as a particulate phase.
In HA-CaHA systems, CaHA microspheres need to enter a gel carrier and then pass through dispersion, extrusion, stability, sterilization, biological evaluation, and quality-documentation processes. Particle-size distribution, sphericity, particle integrity, dense structure, phase composition, and impurity control can all affect how R&D teams interpret the material.
This is especially relevant in the under-eye region, where tissue layers are delicate and visible changes are easier to detect. Clearly defined CaHA microsphere specifications, stable HAp/CaHA raw-material quality, and verifiable 25-45 μm fully solid, dense CaHA microsphere parameters can help reduce unnecessary variables in composite-system development.
Although the cited study focuses on a clinical application, it also points back to material development: particulate materials cannot be evaluated by name alone. Particle-size window, morphology, structure, and batch performance remain part of the development conversation.
Conclusion
Lower-eyelid and tear-trough rejuvenation is moving from simple hollow correction toward more detailed combination-system evaluation. Research on HA combined with CaHA microspheres reflects this shift.
The point is not that one approach has become the standard answer. A more restrained reading is that under-eye rejuvenation increasingly requires material behavior, injection plane, tissue response, and follow-up results to be considered together. For hydroxyapatite microsphere and HAp/CaHA raw-material development, this means material identity, specification window, particle morphology, and quality consistency need to be clearly defined.
This article is intended for industry information and literature review only. It discusses publicly available research and raw-material development trends, and does not provide recommendations for specific medical products, clinical indications, or treatment decisions.
References
Gui Wanli, Zou Qipa. Application of Injectable Sodium Hyaluronate Combined with Hydroxyapatite Microspheres in Lower Eyelid Rejuvenation. Chinese Journal of Aesthetic Medicine. 2026;35(3):63-67. Public abstract: Chinese Journal of Aesthetic Medicine, Issue 3, 2026.