In aesthetic-material and soft-tissue augmentation literature, calcium hydroxylapatite (CaHA) is rarely discussed in isolation. It more often appears as part of a composite system, where CaHA particles are dispersed in carriers such as carboxymethyl cellulose (CMC), hyaluronic acid (HA), and other gel matrices. In these systems, both the particle phase and the carrier phase shape the material behavior.
The carrier influences early dispersion, extrusion behavior, and shape retention. CaHA microspheres, in turn, govern particle distribution, material identity, tissue-interface response, and later evaluation outcomes. Recent publications reflect this split: one line of work examines CaHA/CMC material characterization and animal histology, another discusses HA-CaHA hybrid injectables through expert recommendations, and a third reports 12-month follow-up data from a defined nasal augmentation cohort.
These systems should be kept separate. CaHA/CMC usually refers to CaHA particles dispersed in a CMC-based carrier. HA-CaHA hybrid injectables are typically defined as CaHA microspheres dispersed or embedded in a cross-linked HA gel matrix. Both are CaHA-related composite injectable systems, but their carriers, rheology, and product-design logic are different.
I. What the CaHA/CMC Animal Study Shows
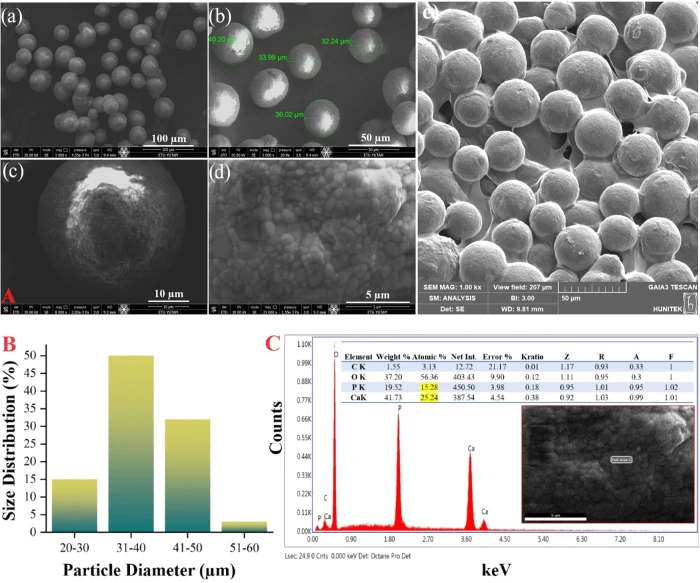
A 2024 study in ACS Omega characterized a Hydroxyapatite/Carboxymethyl Cellulose (CaHA/CMC) matrix and evaluated it in a rat subcutaneous model. The material contained 20–60 μm CaHA ceramic particles dispersed in a carrier made of CMC, glycerin, and water for injection. The study covered material composition, physicochemical characterization, rheology, and histological changes at different time points.
The material data were clearly reported. SEM images showed relatively uniform spherical CaHA particles in the matrix. EDS analysis gave a Ca/P ratio of 1.65, close to the stoichiometric Ca/P ratio of hydroxyapatite (1.67). The authors also included heavy-metal testing as part of the material evaluation.
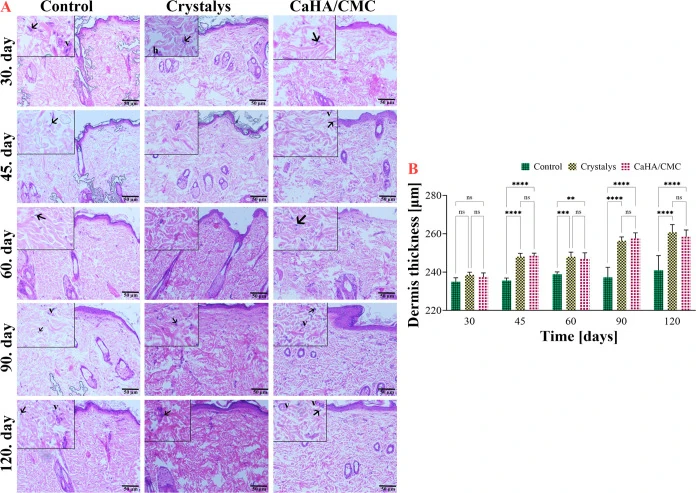
For the animal experiment, 150 μL of sterilized CaHA/CMC was injected subcutaneously into rats and compared with Crystalys and a control group. Tissue samples were collected at 30, 45, 60, 90, and 120 days. The paper reported significant increases in dermal thickness, elastic fibers, and collagen density in the CaHA/CMC group. Based on these findings, the authors described the gel as biocompatible, with potential for soft-tissue repair and augmentation in this animal model.
From a material-development perspective, the useful point is not simply that the formulation contains CaHA. The study separates the system into particles, carrier, rheology, and tissue response. For CaHA-based composites, later evaluation depends on how particles are dispersed, how the gel behaves, and what local tissue changes are observed in the selected model.
II. What the Rheology Data Add
CaHA/CMC systems draw attention partly because of their rheological behavior. For injectable composite materials, rheology is not merely a laboratory metric. It affects particle suspension, extrusion behavior, shape retention, and formulation development.
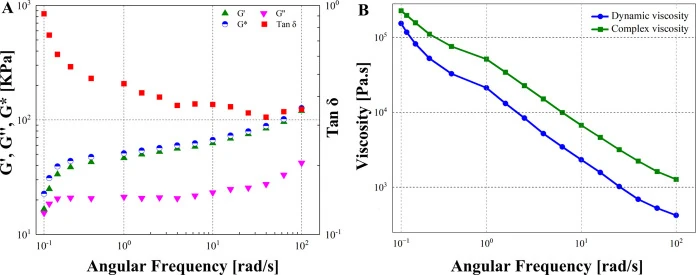
The ACS Omega study reported storage modulus (G′) values of 58.6 kPa at 2 Hz and 68.9 kPa at 5 Hz. The corresponding loss modulus (G″) values were 21.7 kPa at 2 Hz and 24.8 kPa at 5 Hz. Under these test conditions, G′ remained higher than G″, indicating that the elastic response was dominant and that the gel had measurable structural-support behavior.
These values are more useful than a broad statement such as "good support." G′ reflects the ability of a material to store elastic energy under small deformation, while G″ reflects viscous energy dissipation. Together, they help describe how the composite system may hold particles in suspension, resist deformation, and maintain structure in the carrier.
Rheology still has clear limits. In vitro rheological data cannot be treated as a direct substitute for human outcomes. Formulation design, carrier composition, injection depth, operator technique, anatomical site, and tissue differences all affect the final result. Rheology is best used as a material-science basis for formulation screening and comparison.
III. What Animal Histology Can and Cannot Tell Us
Histological sections help show local tissue changes after a material is introduced into tissue. They can reveal inflammatory-cell infiltration, fibrous tissue formation, collagen-related changes, and structural changes around the material.
In the ACS Omega study, H&E staining was used to observe tissue architecture and dermal thickness. VVG staining was used for elastic fibers, and Trichrome staining was used for collagen-related changes. The original Figure 5 presented H&E sections and dermal-thickness statistics over time; Figures 6 and 7 further showed VVG and Trichrome staining results. Together, these figures supported the authors' observations on dermal thickness, elastic fibers, and collagen density.
These results should stay within the animal-model context. A rat subcutaneous model can provide early information on material compatibility and local tissue response, but it cannot be directly extrapolated to human facial anatomy or replace clinical studies.
Animal studies primarily address what local changes may occur after a material is introduced into tissue. Clinical studies evaluate performance in defined populations, anatomical sites, and procedures. The two are related, but they answer different questions.
IV. HA-CaHA Systems in Expert Recommendations
A 2026 expert consensus in the Journal of Cosmetic Dermatology discussed HA-CaHA hybrid injectables for facial rejuvenation. This type of material consists of CaHA microspheres embedded in a cross-linked HA gel matrix. It differs from CaHA/CMC, but it also shows that CaHA-related composite systems are being discussed in more specific application settings.
The consensus is not a primary experimental study. It gathered recommendations from eight international experts on patient selection, skin laxity assessment, injection technique, retreatment, combination treatment, and safety considerations. The panel discussed HA-CaHA use in patients with skin laxity, sagging, and mild-to-moderate volume or contour loss, with an emphasis on structural support and soft-tissue repositioning.
The technical recommendations refer to facial retaining ligaments and the zygomatic arch as anatomical landmarks, favor lateral facial zones, and express a preference for cannulas over needles. These details are not presented here as operating instructions. Their relevance is that HA-CaHA discussion has evolved beyond material classification to encompass anatomy, technique selection, and safety boundaries.
Recommendations for HA-CaHA systems should not be treated as clinical evidence for CaHA/CMC matrices. They are more accurately interpreted as evidence that CaHA microspheres can be combined with different gel carriers, leading to different product designs and evaluation pathways. Such consensus documents should remain tied to their specific product and expert context.
V. A 12-Month Nasal Augmentation Study in Chinese Participants
Also in 2026, the Journal of Cosmetic Dermatology published a 12-month prospective study evaluating calcium hydroxylapatite for nasal augmentation in Chinese participants. The study enrolled 24 female subjects. Three-dimensional facial scanning was used immediately after injection and at 1, 3, 6, 9, and 12 months. The authors also recorded Global Aesthetic Improvement Scale (GAIS) satisfaction scores, pain scores, and local injection-site reactions.
All 24 subjects completed the 12-month follow-up. In the 3D volume analysis, nasal volume decreased between the immediate post-injection time point and 1 month. From 1 to 6 months, volume showed a slight numerical increase that was not statistically significant. At 12 months, the retained volume was 0.94 ± 0.45 mL, significantly lower than at 6 and 9 months. The GAIS responder rate was 79% at 3 months and 58% at 9 months.
The safety profile was reported in detail. Injection-related pain was mild, with a mean Numerical Rating Scale (NRS) score of 1.29 immediately after injection, and resolved within 60 minutes. For local reactions, swelling and tenderness were the most common findings, with 23 cases (60.5%) and 8 cases (21.1%) reported, respectively. All resolved spontaneously within 1 week, and no serious complications were reported in the study.
This study places a CaHA-related material in a defined setting: nasal augmentation, Chinese participants, and 12 months of follow-up. The evaluation therefore moves from material properties to 3D volume change, satisfaction scoring, safety findings, and follow-up outcomes.
It is still a small prospective study focused on one anatomical region. Its results should not be generalized to every hydroxyapatite application. For material development, this type of follow-up shows why particle characteristics, carrier system, application setting, and observation period all matter.
VI. Why Microsphere Specifications Still Matter
Whether the system is CaHA/CMC or HA-CaHA, CaHA microspheres are the key particulate phase. Particle size distribution, morphology, structural density, crystalline phase, surface properties, and trace-impurity control can all affect downstream formulation development and quality evaluation.
The cited studies use concrete metrics: 20–60 μm particle size, Ca/P ratio, G′/G″, in vivo histology, 3D volume measurements, GAIS responder rates, and adverse-event records. For material and formulation teams, these are more useful than broad claims about whether a material is "good."
Microspheres cannot simply be added to a composite gel without further evaluation. They need to match the carrier system, tolerate sterilization and processing, remain well dispersed, support the target rheological profile, and behave consistently during extrusion and biological testing. A broad particle-size window, unstable morphology, or large batch variation can add unnecessary variables to product development.
This is where clear microsphere specifications matter. They provide a defined and reproducible material basis for later formulation work. For teams working on composite hydrogels, soft-tissue augmentation systems, local delivery platforms, or regenerative aesthetic formulations, well-characterized CaHA microspheres, HAp/CaHA raw materials, and a 25–45 μm specification for solid, fully dense microspheres can help reduce avoidable sources of development variability.
VII. Conclusion
From a CaHA/CMC rat model to HA-CaHA expert recommendations and a 12-month nasal augmentation follow-up study, CaHA-related composite systems are being evaluated in increasingly specific ways.
The publications do not support one broad conclusion for all systems. They show different levels of evaluation: material characterization through particle size, Ca/P ratio, and rheology; animal evaluation through dermal thickness, elastic fibers, and collagen-related staining; expert discussion through patient selection and safety boundaries; and clinical observation through volume change, GAIS response, and local reaction records.
These findings should not be read as proof that one raw material or one formulation covers all application settings. A more practical reading is that CaHA composite-system evaluation is becoming more concrete: the material must be clearly characterized, the system must be tested in a defined model, and application-specific follow-up data need to be interpreted within their limits.
For HAp/CaHA material development, this points back to the basics: clear material identity, stable specification windows, and reproducible batch performance. The more stable the base microsphere material is, the easier it becomes to build reliable formulation development and quality evaluation around it.
This page is intended for industry information and literature review only. It discusses publicly available studies and hydroxyapatite material-development trends, and does not provide medical product recommendations, clinical indications, or treatment advice.
References
- Karatas E, Koc K, Yilmaz M, Aydin HM. Characterization and Comparative Investigation of Hydroxyapatite/Carboxymethyl Cellulose (CaHA/CMC) Matrix for Soft Tissue Augmentation in a Rat Model. ACS Omega. 2024;9(29):31586–31600. DOI: 10.1021/acsomega.4c01503.
- Cavallini M, et al. Global Recommendations for Facial Rejuvenation Using a Hyaluronic Acid and Calcium Hydroxyapatite Hybrid Injectable. Journal of Cosmetic Dermatology. 2026;25(1):e70608. DOI: 10.1111/jocd.70608.
- Wang J, et al. Efficacy and Safety of Calcium Hydroxylapatite for Nasal Augmentation: A 12-Month Prospective Study in a Chinese Population. Journal of Cosmetic Dermatology. 2026;25(4):e70862. DOI: 10.1111/jocd.70862.